


The Use of Stimulants in Russian Armed Forces Units
The Main Military Medical Directorate of the Russian Ministry of Defense has issued methodological guidelines on the pharmacological adjustment of servicemen’s performance. These guidelines describe the use of stimulants to enhance the combat effectiveness of military personnel.
The primary danger of such substances lies in the fact that they do not eliminate physical exhaustion but merely mask it, leading to rebound effects, psychological dependence, nervous breakdowns, and a decline in real combat readiness.
Researchers from Russia’s Main Military Medical Directorate have developed a so-called “pharmacological correction program”, allowing for the continuous intake of medications throughout the entire duration of a combat mission.
The Russian military’s “combat first-aid kit” includes the drugs “Loksidan” and “UR-1.”
Loksidan is a combination of the stimulants bromantane and mesocarb (an amphetamine derivative). It is intended to temporarily suppress fatigue and drowsiness while increasing physical endurance, allowing soldiers to function for up to two days without sleep.
UR-1 is an experimental drug based on modafinil, a substance known for its use in the armed forces of the United States, France, and the United Kingdom. UR-1 is designed primarily for cognitive stimulation, enhancing clarity of thought, reaction speed, and attention. While modafinil has indeed been used by the U.S., French, and Canadian militaries, this was done only under strict medical supervision. The Russian approach, by contrast, involves mass and systematic use.
Both drugs are officially used only in Russia and are presented as tools for airborne troops, special forces, and naval infantry. In addition to this so-called “elite combat kit,” Russian military medics have developed 14-day stimulant programs for regular soldiers, including meldonium, fonturacetam, and Noopept—nootropic substances intended to improve memory and concentration. All of these drugs are commercially available in civilian pharmacies and are not classified as potent controlled substances, which simplifies their distribution and use.
The fundamental problem with these “combat schemes” is that the drugs do not address actual fatigue but merely conceal it. The body is pushed to its physiological limits, followed by a sharp “crash” characterized by exhaustion, nervous breakdowns, sleep disturbances, and blood pressure instability. Psychological dependence also develops: soldiers begin to believe they are incapable of performing tasks without chemical support. This creates a self-reinforcing cycle, in which pharmacological stimulation substitutes for genuine training.
Thus, the Russian army relies not only on mobilization and propaganda, but also increasingly on pharmacology. However, the pills issued to soldiers—and even to prisoners before deployment to the front—do not turn them into “super-soldiers.” They provide a short-term effect, while in the long term undermining health and combat capability.
Attempting to sustain combat effectiveness through chemical means is short-sighted and dangerous. True military effectiveness rests on training, morale, proper logistical support, and leadership, not on pharmacological stimulation.
2. Soviet Precedents: Stimulants as a Tool of Mass Armies
2.1 World War II: Amphetamines and Forced Endurance
During the Second World War, the Red Army, like many other armies, used amphetamine-based stimulants (primarily phenamine) to:
- Extend marching endurance,
- Maintain wakefulness during prolonged operations,
- Support night assaults and forced advances.
These substances were widely distributed among reconnaissance units, tank crews, pilots, and shock infantry formations. While short-term performance gains were recorded, Soviet military medical archives document:
- Sharp post-combat exhaustion,
- Increased rates of cardiovascular collapse,
- Elevated incidents of indiscipline and impulsive behavior.
Importantly, stimulant use was situational, not continuous, and generally limited to specific phases of offensive operations.
2.2 Cold War Era: Aviation, Special Forces, and “Functional Readiness”
In the post-war period, the Soviet Armed Forces institutionalized pharmacological support under the doctrine of “functional readiness.” This included:
- Psychostimulants for long-range bomber crews,
- Sedatives and counter-stimulants to manage sleep cycles,
- Nootropic experimentation to improve operator focus.
However, even in the late Soviet system, usage was:
- Medically supervised
- Restricted to specific professional categories
- Explicitly time-limited
Soviet military medicine recognized that continuous stimulant use reduced operational reliability, especially under stress and combat losses.
2.3 Afghanistan (1979–1989): Combat Fatigue and Chemical Compensation
During the Afghan war, stimulant use expanded informally:
- Among airborne and motorized rifle units,
- During prolonged mountain operations,
- In conditions of chronic sleep deprivation
Veteran testimonies and post-war medical assessments highlight:
- Rising dependency on stimulants and alcohol,
- Severe post-combat psychological disorders,
- Long-term degradation of unit cohesion.
Crucially, Soviet planners concluded that chemical compensation could not offset poor logistics, morale erosion, or unclear political objectives.
3. What Is Different in the Russian Case
The modern Russian approach diverges from Soviet precedent in three critical ways:
3.1 From Situational to Systemic Use
Where the Soviet Army used stimulants episodically, Russia is normalizing continuous intake throughout combat missions, including for:
- Mobilized personnel
- Poorly trained conscripts
- Convicts recruited from prisons
This marks a shift from medical support to biological exploitation of manpower.
3.2 Absence of Medical Oversight
Unlike NATO forces—where modafinil use is rare, optional, and strictly monitored—the Russian system:
- Distributes stimulants en masse,
- Lacks individualized dosage control
- Treats side effects as acceptable attrition.
This increases the probability of:
- Sudden cardiovascular events,
- Cognitive collapse under stress,
- Friendly-fire incidents and command breakdowns.
Pharmacology Replacing Training
Perhaps most critically, pharmacology is being used to compensate for structural failures:
- Insufficient training cycles,
- Poor morale,
- Equipment shortages,
- Leadership deficits.
This mirrors late-Soviet decline patterns, but under far worse operational pressure.
Operational and Strategic Consequences
Short-Term Effects
- Temporary endurance increase,
- Suppressed fear and fatigue,
- Artificial stabilization of front-line performance.
Medium-Term Effects
- Rising psychological dependency,
- Increased medical evacuations,
- Loss of initiative and adaptability.
Long-Term Effects
- Irreversible health damage,
- Collapse of unit cohesion,
- Declining combat reliability despite numerical presence.
Historically, armies that rely on chemical stimulation rather than institutional strength exhaust themselves faster, even if tactical performance briefly improves.
Strategic Assessment
Pharmacological stimulation is a symptom of systemic weakness, not a force multiplier.
From the Red Army in World War II to Soviet forces in Afghanistan, historical experience shows that stimulants cannot substitute for training, morale, logistics, and leadership. Russia’s current reliance on pharmacology reflects:
- Manpower exhaustion,
- Operational overextension,
- The erosion of professional military culture.
In the long run, this approach accelerates degradation rather than preventing it, turning short-term endurance into long-term collapse.
Strategic Consequences of Pharmacological Stimulation in the Russian Armed Forces
Pharmacological stimulation can temporarily delay military failure, but it cannot generate strategic advantage. Over time, it accelerates force degradation, increases command risk, and undermines Russia’s ability to sustain prolonged war.
What Russia CAN achieve (short-term, tactical–operational)
Temporary manpower amplification
- Enables overstretched units to hold positions longer
- Extends endurance during:
- prolonged defensive battles,
- night assaults,
- emergency rotations with insufficient rest.
- Compensates for numerical losses without immediate reinforcement
Strategic effect:
Buys time for political decisions, mobilization cycles, or defensive stabilization.
Masking systemic exhaustion
- Conceals real levels of fatigue from:
- commanders
- planners
- political leadership
- Maintains the illusion of operational resilience
Strategic effect:
Allows the Kremlin to sustain war narratives and delay recognition of structural failure.
1.3 Increased short-term aggression
- Lowers fear thresholds,
- Increases risk-taking and impulsive assaults,
- Can temporarily raise assault intensity.
Strategic effect:
Useful for attritional warfare, where shock value matters more than survivability.
What Russia CANNOT achieve (strategic limits)
No improvement in real combat effectiveness
Stimulants do not improve:
- tactical judgment,
- coordination under fire,
- adaptive decision-making,
- leadership quality
In complex combat environments, chemically overstimulated troops:
- misread threats,
- overreact,
- break discipline under stress,
Strategic reality:
War is won by coherence, not wakefulness.
2.2 No substitute for training or professionalism
Pharmacology cannot replace:
- combined-arms integration,
- NCO initiative,
- mission command,
- unit cohesion.
Historical pattern (Soviet → Russian):
Chemical stimulation rises as training quality falls.
Medium-term strategic consequences (negative)
3.1 Accelerated force burnout
- Post-stimulation “crashes” cause:
- sudden combat ineffectiveness,
- medical evacuations,
- desertions and refusals.
- Units become operationally unreliable within months
Strategic cost:
Russia loses predictability of force output, complicating planning.
Command-and-control degradation
Stimulant use increases:
- emotional volatility,
- tunnel vision,
- friendly-fire risk,
- disobedience or panic under pressure.
Strategic cost:
Higher probability of localized collapses, even without enemy breakthroughs.
Psychological dependency and morale erosion
Soldiers internalize the belief:
“Without pills, I cannot fight.”
This:
- undermines confidence,
- weakens intrinsic motivation,
- replaces discipline with chemical reliance.
Strategic cost:
Long-term morale collapses faster than casualty rates would predict.
Long-term strategic consequences (systemic damage)
Permanent loss of trained manpower
- Cardiovascular damage,
- Neurological disorders,
- PTSD amplification,
- Reduced veteran reusability.
Strategic cost:
Russia’s force regeneration capacity deteriorates irreversibly.
Institutional decay of military culture
Pharmacological dependence signals:
- acceptance of expendability
- erosion of duty of care
- collapse of professional ethics
Strategic cost:
The army becomes a consumable instrument, not a sustainable institution.
Adverse selection of leadership
- Leaders who tolerate chemical overstimulation rise;
- Leaders who demand training and rest are sidelined.
Strategic cost:
Future command corps becomes risk-blind and politically loyal, not competent.
Strategic comparison: what pharmacology reveals about Russia’s war posture
| Indicator | Interpretation |
| Systemic stimulant use | Manpower exhaustion |
| Continuous intake | Prolonged high-intensity attrition |
| Use on mobilized & convicts | Collapse of professional core |
| Lack of medical oversight | Acceptance of irreversible losses |
| Replacement of rest/training | Strategic desperation |
Bottom-line strategic conclusion
Pharmacological stimulation is a delaying tactic, not a force multiplier.
It allows Russia to:
- postpone operational collapse,
- sustain pressure temporarily,
- maintain political narratives.
But it guarantees:
- faster long-term degradation,
- lower adaptability,
- loss of strategic endurance.
In strategic terms, Russia is converting biological capital into time—
and time into irreversible weakness.
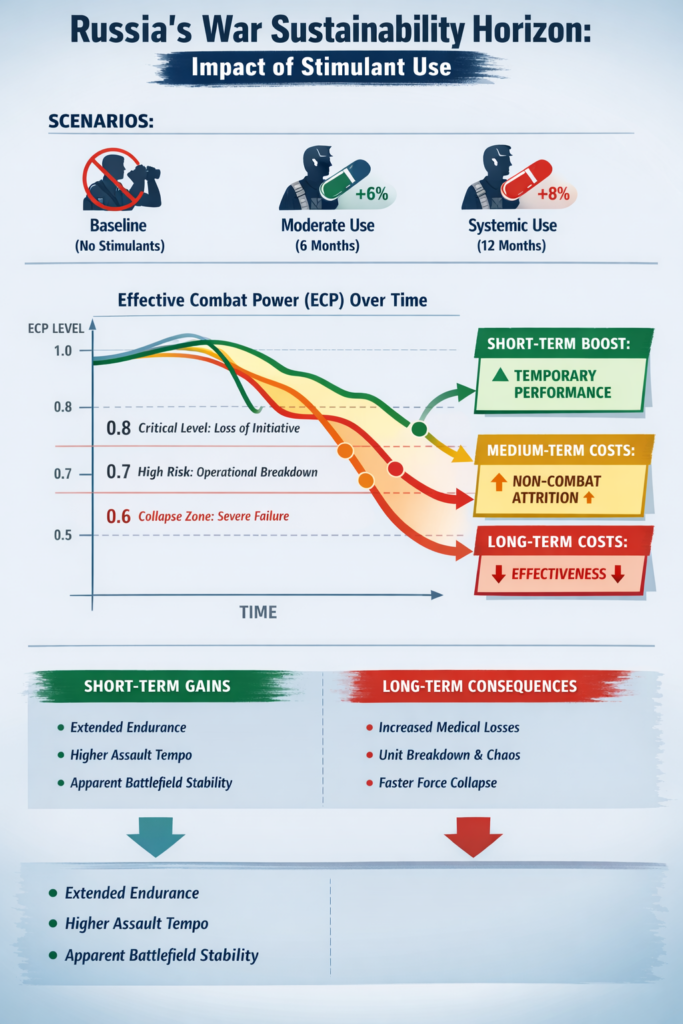
effective combat power (ECP) below which the force can’t sustain its current operational posture.
Common analytic thresholds:
- 0.8 = “can still fight, but loses initiative; defense becomes brittle”;
- 0.7 = “operational failure risk rises sharply; rotations and reserves stop working”;
- 0.6 = “systemic collapse in sector(s); large withdrawals likely”.
Core model: Effective Combat Power
Model ECP as:
Where:
- N(t) = available personnel (not just on paper—available, deployable, not medically sidelined)
- E(t) = effectiveness per soldier (fatigue, cognition, discipline, initiative)
- L(t) = leadership/logistics multiplier (ammo, comms, medevac, command cohesion)
Stimulants mostly affect E(t) short-term, but they also increase attrition and degrade L(t) over time (more med cases, accidents, discipline issues).
How stimulants change the system
Immediate effect (weeks)
- E(t) increases temporarily (wakefulness, reduced perception of fatigue)
Delayed effects (months)
- Non-combat attrition rises (cardio events, sleep collapse, psych episodes, injuries from risk-taking)
- Effectiveness decays faster (crash cycles, dependency, degraded judgment)
- Leadership/logistics burden rises (more medical evacuations, more discipline incidents)
So your model should include two penalties:
- Extra non-combat attrition
- Extra effectiveness decay
A worked example (illustrative)
Assume a force tries to hold a high-intensity front with:
- Initial N₀ = 400,000
- Monthly combat losses 4%
- Monthly baseline non-combat attrition 1.5%
- Monthly replacements 20,000
- Baseline effectiveness decay from fatigue/rotation limits 1.5% per month
Now compare three policies:
A) No systemic stimulant program
Baseline attrition and fatigue only.
B) “Moderate” systemic stimulant use (6 months)
- Temporary performance boost: +6% while used
- Extra non-combat attrition: +1.2% / month (medical + accidents + breakdowns)
- Extra effectiveness decay: +1.2% / month (crash/instability)
C) “Systemic” stimulant use (12 months)
- Temporary performance boost: +8%
- Extra non-combat attrition: +2.0% / month
- Extra effectiveness decay: +2.0% / month
Result: sustainability horizon (time to cross thresholds)
Using the model above, the time to fall below ECP thresholds:
| Threshold | No stimulants | Moderate (6 mo) | Systemic (12 mo) |
| 0.8 | ~13 months | ~7 months | ~5 months |
| 0.7 | ~21 months | ~12 months | ~7 months |
| 0.6 | >24 months | ~22 months | ~10 months |
Interpretation: stimulants can make units look functional early, but they pull the horizon forward by accelerating medical attrition and coherence loss.
Why the “boost” doesn’t save the horizon
Even if stimulants give +6–8% short-term performance, they typically add:
- more people leaving the line (medical/behavioral attrition)
- more mistakes per operation (discipline, friendly-fire risk, navigation errors)
- more command load (medevac, crisis management)
In the model, E(t) benefits are linear and temporary; attrition + decay penalties compound. Compounding wins.
What this means strategically for Russia
If systemic stimulant use expands, Russia can achieve:
- Short-term front stabilization (weeks–months)
- Higher assault tempo for short windows
- Narrative continuity (“we’re holding; we’re advancing”)
But it tends to produce:
- Earlier operational exhaustion point
- More sectoral collapses (units “drop off a cliff” after crash cycles)
- Lower force regeneration quality (returning soldiers less reusable; training replaced by chemical bridging)
- Higher command brittleness (cohesion fails under shock)
Net: Russia trades biological capital for time—and time for irreversible degradation.

